The indications for
and results of HDR afterloading therapy in diseases
of the skin and mucosa with standardized surface
applicators (the
Leipzig
applicator)
Köhler-Brock
A,
Strahlenther Onkol. 1999 Apr;175(4):170-4
Klinik und Poliklinik für
Strahlentherapie und Radioonkologie, Universität
Leipzig.
BACKGROUND:
In our department we have developed a standardized
applicator for HDR brachytherapy of surface lesions,
the so called Leipzig-applicator. We have used this
method since September 1987, initially with a
Decatron remote afterloading machine, but more
recently from November 1990 with a microSelectron-HDR.
We report about our experience of 10 years. PATIENTS
AND METHOD:
Since 1987 we
treated 520
patients in 3,026 fractions with this method.
In most of the cases we irradiated tumors of the
skin of the face, but we also treated tumors of the
mouth, of the tongue, of the perianal region and the
external genitalia. The histological types were in
most of the cases squamous cell carcinomas and basal
cell carcinomas, but we also treated tumors like
Kaposi-sarcomas, melanomas and skin manifestations
of lymphomas and solid organ tumors. We also
irradiated benign lesions like keloids after
excision. We use single doses between 5 and 10 Gy
once to twice a week. The isodose distribution was
depending of the tissue infiltration of the tumor.
The total dose was 30 to 40 Gy. RESULTS:
In 91% of
the cases we obtained a complete remission of
the tumor, in 6% a partial remission. Recurrences
appeared in 8% of the patients. In most cases the
reason of the recurrence was a lower brachytherapy
dose because of a prior radiotherapy.
We didn't
observe any severe late radiation reaction.
CONCLUSION: We consider that our series of patients
treated with HDR brachytherapy and a range of
standardized applicators demonstrates that this is a
successful method of treating surface lesions.

{kind=link}
{kind=link}

 Valencia isodose pattern
Valencia isodose pattern
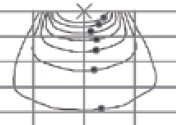 Leipzig isodose
Leipzig isodose