| Etiology
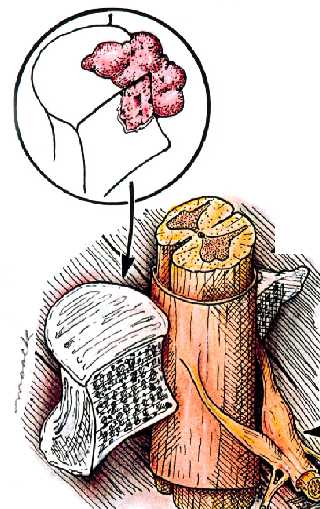
Compression of the spinal cord is due predominantly to extradural metastases (95%) and
usually results from tumor involvement of the vertebral column (see pic.) A tumor may
occasionally metastasize to the epidural space without bony involvement.
Site of involvement The segment most often involved is the thoracic spine (70%), followed
by the lumbosacral (20%) and cervical spine (10%).
Most common malignancies Although spinal cord compression occurs in a variety of
malignancies, the most common are lung, breast, unknown primary, prostate, and renal
cancers, as well as lymphoma and myeloma.
Signs and symptoms
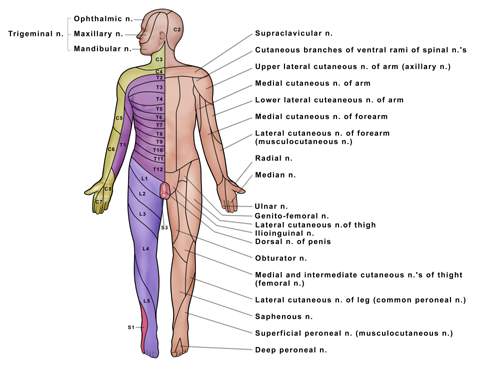
Early signs Over 90% of patients present with pain radicular in nature (ie, not due to
bone involvement but rather due to neural compression), which may be localized to the
spine or radicular in nature (pain or numbness follows a dermatome
pattern see
diaagram#1
and
diagram #2 and diagram #3.) Pain, which is
usually secondary to bony involvement, is often exacerbated with movement, recumbency,
coughing, sneezing, or straining. The majority of patients experience pain for weeks to
months before neurologic symptoms appear.
Intermediate signs If cord compression goes untreated, weakness often develops next. It
may be preceded or accompanied by sensory loss.
Late signs Symptoms of autonomic dysfunction, urinary retention, and constipation are late
findings. Once autonomic, motor, or sensory findings appear, spinal cord compression
usually progresses rapidly and may result in irreversible paralysis in hours to days if
untreated.
Physical findings may include tenderness to palpation or percussion over the involved
spine, pain over the involved vertebra or in the distribution of the involved nerve root,
muscle weakness, spasticity, abnormal muscle stretch reflexes and extensor plantar
responses, and sensory loss. Sensory loss occurs below the involved cord segment and
indicates the site of compression. In patients with autonomic dysfunction, physical
findings include a palpable bladder, a large volume of residual urine postvoiding, or
diminished rectal tone.
Diagnosis
The first step in the diagnosis of spinal cord compression is an accurate neurologic
history and examination.
X-rays A plain radiograph of the spine may be helpful. More than 66% of patients with
spinal cord compression have bony abnormalities on plain radiographs of the spine.
Findings include erosion and loss of pedicles, partial or complete collapse of vertebral
bodies, and paraspinous soft-tissue masses. Normal spine films are not helpful for
excluding epidural metastases.
MRI The standard for diagnosing and localizing epidural cord compression is the MRI scan.
Gadolinium-enhanced MRI has been especially helpful in assessing cord compression
secondary to spinal epidural abscesses, as gadolinium enhances actively inflamed tissues
and defines anatomic boundaries. An abnormal signal within the disk space suggests the
possibility of infection. MRI with gadolinium enhancement also has been useful in
evaluating thoracic spinal cord compression.
Primary or secondary neoplasms involving the vertebral bodies generally demonstrate a long
T1, resulting in decreased signal intensity on T1-weighted image, and a long T2,
with increased signal intensity of the T2-weighted image.
CT and myelography If MRI is unavailable, a CT scan and/or myelogram may be used to
diagnose and localize epidural cord compression.
Prognosis
Treatment outcome correlates with the degree of neurologic impairment prior to therapy. In
a prospective analysis of 209 patients treated for spinal cord compression with
radiotherapy and steroids, Maranzano and Latini reported that, of patients who were
ambulatory, nonambulatory or paraplegic prior to treatment, 98%, 60%, and 11%,
respectively, were able to ambulate following therapy. Treatment outcome was superio in
the most radiosensitive malignancies (eg, lymphoma, myeloma) than in the less sensitive
cancers (renal cell carcinoma, hepatoma). Almost all ambulatory patients treated with
either radiation alone or laminectomy followed by postoperative radiation remained
ambulatory after treatment, qhereas ~10% of patients whose lower extremities were
paralyzed could walk after treatment.
Treatment
The goals of treatment of spinal cord compression are recovery and maintenance of normal
neurologic function, local tumor control, stabilization of the spine, and pain control.
The choice of treatment depends on the clinical presentation, availability of histologic
diagnosis, rapidity of the clinical course, type of malignancy, site of spinal
involvement, stability of the spine, and previous treatment.
Radiation therapy
Radiation therapy alone is now the standard initial treatment for most patients with
spinal cord compression due to a radiation-sensitive malignancy. Treatment outcome is
contingent upon both the relative radiosensitivity of the malignancy and the neurologic
status of the patient at the time radiotherapy is initiated.
Maranzano and Latini treated 53 consecutive patients, from 1993 to 1995, with 800 cGy × 2
(to 1,600 cGy) given over 2 weeks. At a median follow-up of 25 months (range, 6-34
months), 67% of the patients experienced pain relief, and 63% showed improvements in motor
function. No late toxicities were reported. This regimen was suggested for patients with
less “radio-responsive” tumors (eg, NSCLC, renal cell sarcinoma, melanoma,
sarcoma) or those with paralysis or short life expectancy. The reg-imen was similar to 300
cGy × 10 in terms of symptom relief, surviv-al, and duration of response, regardless of
tumor histology.
Radiation portal In general, the treatment volume should include the area of epidural
compression (as determined by MRI or myelography) plus two vertebral bodies above and
below. Consideration should be given to including adjacent areas of abnormalities if
feasible. Careful matching techniques should be employed in patients treated to adjacent
vertebral levels, a situation that is not uncommon.
Radiation dose and fractionation The optimal dose and fractionation scheme has not been
determined. The chosen regimen should take into account such factors as field size and
normal tissue tolerance. Smaller fields are appropriately treated to 2,000-3,000 cGy over
1 or 2 weeks, respectively. Larger fields may occasionally necessitate longer courses,
such as 4,000 cGy over 4 weeks, to minimize side effects.
Retreatment may be entertained, particularly when no effective alternative exists.
Usually, doses of 2,000 cGy over 2 weeks can be used for retreatment. It is important,
however, to counsel the patient regarding the risk of radiation myelopathy. Furthermore,
only those patients who had a lasting response to the initial treatment should be
reirradiated, as tumors that were refractory to the first course or that recur within 3
months are unlikely to respond to subsequent courses.
Steroids
Dexamethasone should be administered if the patient’s history and neurologic
examination suggest spinal cord compression. High-dose IV dexamethasone (100 mg), followed
by 4 mg every 6 hours, may produce rapid relief of pain and improved neurologic function.
However, 10 mg of dexamethasone via intravenous push is used most commonly.
Surgery
Vertebral body resection for tumor anterior to the cord and posterior laminectomy for
tumor posterior to the cord may be appropriate treatment options for relieving spinal cord
compression in patients who require spinal stability, have undergone previous radiotherapy
in the area of the compression, require a tissue diagnosis of malignancy, or experience
progression of the cord compression despite optimal treatment with steroids and radiation.
In general, surgical decompression should be strongly considered in patients whose cord
compression is caused by a relatively radioresistant cancer and who have a severe
neurologic deficit (such as bowel or bladder dysfunction). Unfortunately, many patients in
this situation are not candidates for aggressive surgery. In these cases, radiotherapy is
offered, albeit with limited expectations for neurologic recovery.
Chemotherapy
Chemotherapy may be an effective treatment for spinal cord compression in very select
patients with a chemosensitive metastatic tumor. It also may be considered in combination
with other treatment modalities, such as radiotherapy, or as an alternative if those
modalities are not suitable options for relieving cord compression. |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}